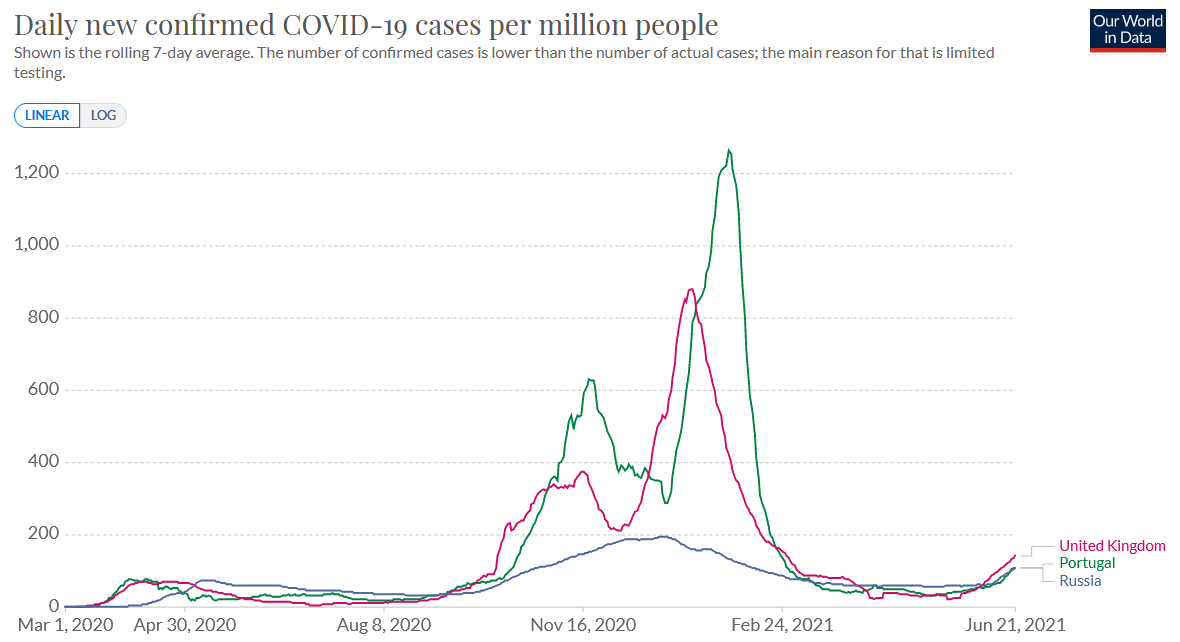
Summer wave driven by the ‘Indian variant’ (delta) in the UK, Russia and Portugal (OWD)
Published: June 22, 2021 Share on: Twitter / Facebook Select LanguageCzechDutchEnglishFrenchGermanGreekHebrewHungarianItalianJapaneseKoreanPolishPortugueseRussianSpanishSwedishTurkishPowered by
On the ‘Indian variant’ summer wave and the mysteries of respiratory virus seasonality.
Since April/May 2020, when coronavirus infections temporarily vanished even in countries with almost no “interventions” (such as Sweden), it has been quite clear that transmission of the novel coronavirus is primarily determined by seasonal influences, similar to influenza viruses and other human coronaviruses (see charts below).
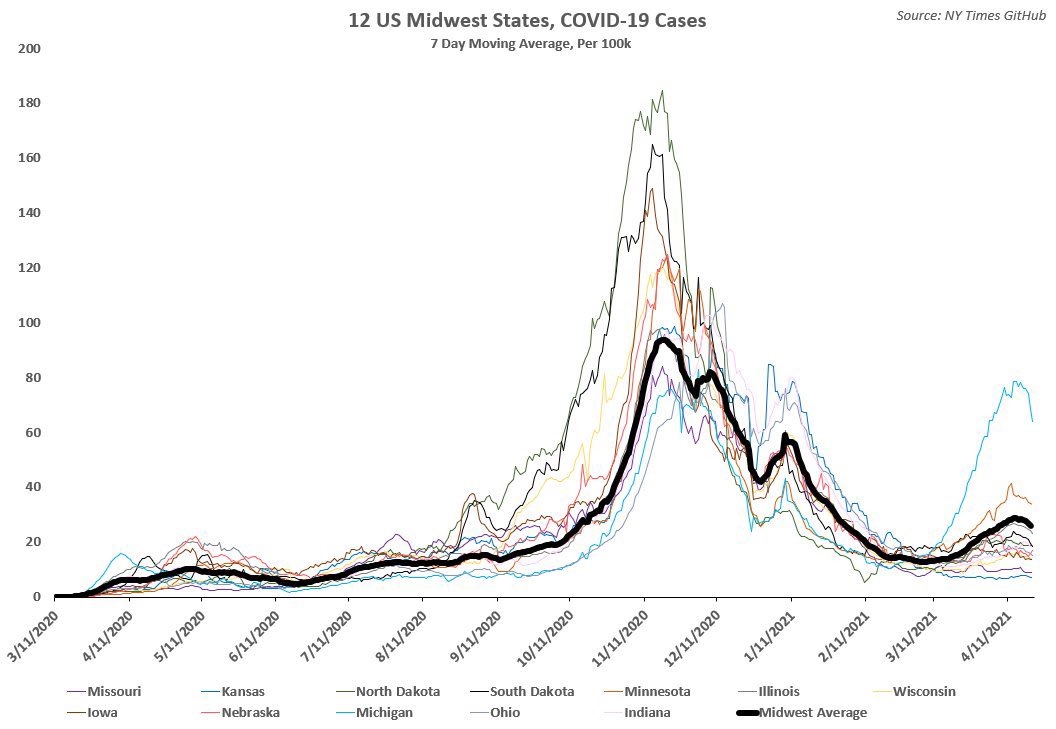
This assessment has later been confirmed by the stunning synchronicity of coronavirus infection rates in neighboring US and European states with entirely different “covid policies” (e.g. concerning face masks, school closures and business closures). Thus, most health authorities have dramatically overestimated the impact of their coronavirus policies (see charts below).
Interestingly, however, the new ‘Indian variant’ of the coronavirus (delta) appears to be the first major exception to this seasonal pattern (1). In the three northern hemisphere countries in which it has already established itself (and only in these!) – the UK, Portugal and Russia – infections in June have markedly increased (see chart above).
In the highly-vaccinated UK, the impact on hospitalizations appears to be limited so far, but Portugal and Russia – especially Moscow – report a significant strain on their health care systems and have already re-imposed new (partial) lockdowns (Russia has already lost 500,000 people to covid). Moreover, China and even Israel are also reporting new outbreaks driven by the Indian variant.
Respiratory virus transmission and seasonality
Is is important to note that while the seasonality of many respiratory viruses is well established (see charts below), virologists and epidemiologists still do not understand the factors driving this phenomenon, which is why their models fared so poorly during the covid pandemic.
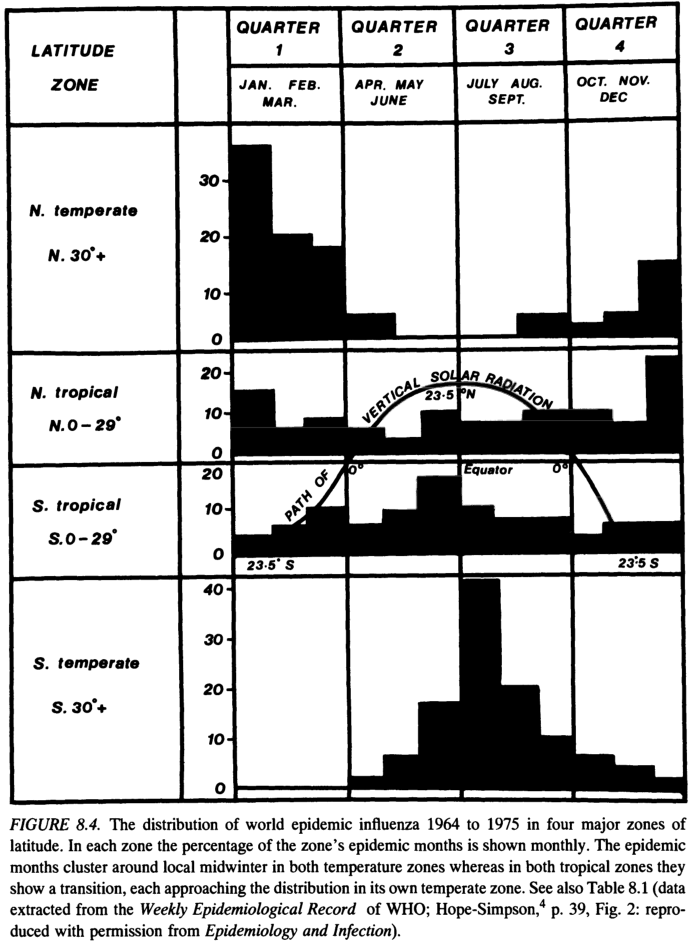
Animal studies have shown that both temperature and relative humidity influence aerosol transmission, essentially bringing infections to a stop at high temperatures or high relative humidity (2). But this doesn’t explain respiratory virus transmission dynamics in the tropical and sub-tropical regions, which have never followed a typical seasonal pattern anyway (see charts below).
Thus, transmission dynamics in countries like Brazil have not been a valid counter-argument to well-established seasonality in moderate climate zones in the northern and southern hemispheres. The deeper issue here is that not only do we not understand the seasonality of respiratory viruses, but we do not even really understand virus transmission itself. (3)
The WHO initially emphasized the role of droplet transmission, triggering the face mask frenzy, but droplet transmission seems to be the least likely route, only relevant if people kiss each other or cough each other into the face, as droplets by definition cannot be inhaled.
The WHO also emphasized the role of fomite transmission (transmission via surfaces of objects, such as doorknobs), triggering the mass disinfection and “wash your hands” frenzy. Studies have confirmed that on some surfaces (including FFP2/N95 masks, by the way), the coronavirus may survive for several hours or even days. Nevertheless, so far no study has found fomite transmission to be a major route of real-world coronavirus infections (but it still might be).
In contrast, respiratory aerosols are likely a major route of coronavirus transmission, and they could explain the importance of indoor vs. outdoor transmission, the failure of facemasks, seasonality, and the higher transmission by adults vs. children and obese vs. lean people. (4)
In addition, infectious coronavirus has been shown to be present in feces, and fecal viral shedding may occur even after respiratory shedding already stopped. This enables transmission via the direct fecal-oral route (e.g. traces of fecal matter on food, in water, or transmitted by flies) and also via the fecal-aerosol route (when flushing the toilet).
While the direct fecal-oral route probably doesn’t play a major role in Western countries (although it was a major transmission route of the polio virus), the fecal-aerosol route has been confirmed in both SARS-1 and SARS-2 outbreaks and has been responsible for mysterious “no contact” transmission between multiple apartments connected via ventilation or sewage water systems.
Thus, public and private toilets are likely places of very high transmission risk and might in part explain off-season outbreaks. Interestingly, the only country that seriously tackles fecal-aerosol transmission has been China, which introduced the notorious “anal swab” testing technique and asks quarantined visitors to use disinfectant when flushing the toilet.
At any rate, the ‘Indian variant’ summer wave is real and highlights the importance, especially in high-risk people, of considering either experimental vaccines or early outpatient treatment.
Most recently, a series of randomized, double-blinded and placebo-controlled trials in Brazil found that proxalutamide – an anti-androgen drug, blocking male sexual hormones and thus inhibiting androgen-driven SARS-2 cell receptors – reduced hospitalization rates in male patients by 91%, while mortality in hospitalized patients (male and female) was reduced by 78%. (5)
Notes
Previous influenza pandemics have shown that novel viruses often have off-season transmission advantages. Most recently, the 2009 swine flu achieved major outbreaks during the summer months of 2009, and largely faded away by November 2009. Thus, summer waves aren’t unprecedented, and do not refute general seasonality.
Interestingly, the original outbreak of the ‘Indian variant’ in India, in April and May 2021, occurred precisely during the time of lowest relative humidity, and prior to the monsoon season.
Because of this, we also don’t understand how respiratory viruses can displace each other on entire continents within just a few weeks, e.g. the novel coronavirus displacing influenza viruses and new coronavirus variants displacing previous coronavirus variants.
SPR previously argued that the ‘Indian’ coronavirus variant may have gotten better at transmitting from younger and leaner people.
The SPR early treatment protocol currently includes prescription-free cough medication bromhexine, which targets the same TMPRSS2 cell receptor used by SARS-2.
Figures
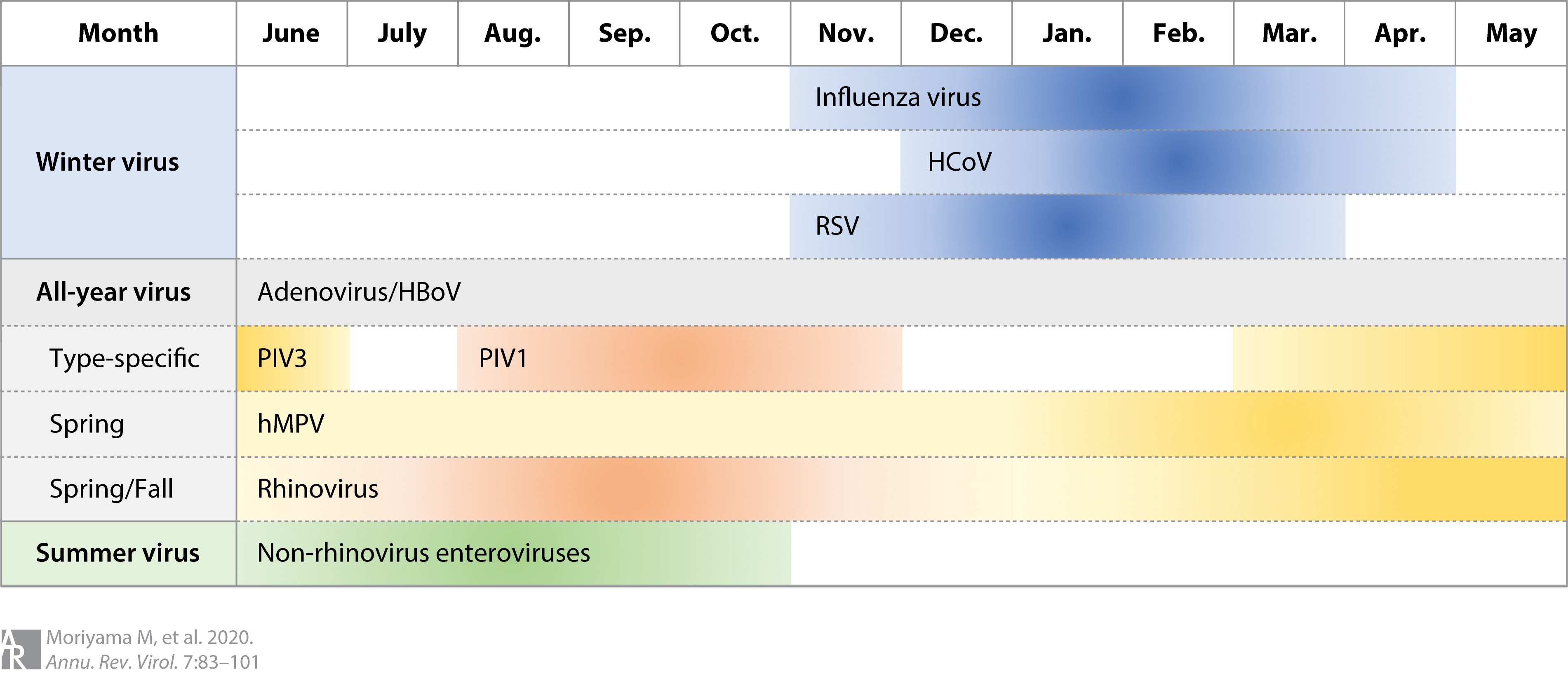
1) Seasonality of respiratory viruses
Seasonality of respiratory viruses
2) Covid-19: Seasonality in US Midwest states
Covid-19: Seasonality in US Midwest states
3) Influenza: Sasonality and dependency on latitude
Just to be clear: as of this time, there is no such thing as a “coronavirus (COVID) vaccine.” That means that, technically, any “information” about such a vaccine, whether positive or negative, claiming it to be either safe or unsafe, can be viewed as factual falsehood and ultimately, a conspiracy theory – since conspiracy theories are typically based on insufficient evidence, yet are promoted as self-evident truths.
But YouTube has announced that it will only clamp down on content that is negative or suspicious about some future vaccine. That means that if you were to make a video praising this non-existent thing and upload it to the platform, that would be fine – however unproven and unprovable at this moment.
It’s not like this hasn’t happened before: at various times, patently harmful substances like DDT were promoted as life-saving epidemic drugs. Even though this DDT clip is positive in tone, in the fullness of time, it clearly reads like a dark conspiracy.
Back to the present, and Reuters is reporting that Google’s video behemoth has decided to add “coronavirus vaccine misinformation” to its lengthy list of topics regarding the catastrophic health scare that have become the subject of meticulous, and at times, unprecedented censorship on the platform.
The way YouTube phrased it in a company blog post on Wednesday is that content about vaccine(s) will be banned if it goes against “consensus” that exists between “local” – i.e., national – healthcare authorities, and the global one, the World Health Organization (WHO).
Specifically, content that expresses suspicion the vaccine might have grave consequences on human health, all the way up to killing people. (Once again, while there is value in not helping spread any kind of unsubstantiated panic, Google/YouTube/WHO at present really have no way of knowing that a future vaccine might not in fact cause harm – this is all yet to be determined.)
But YouTube is already hard at work, with more than 200,000 videos about “Covid misinformation” removed from the platform.
For now at least – “general discussions about broad concerns over the vaccine” are still allowed.
But then again, YouTube in the same breath announced that more censorship around the coronavirus pandemic would be coming soon, “to emphasize authoritative information” – so we’ll just have to wait and see what gets banned next.
Facebook has removed a popular, rapidly growing group where members would post stories about alleged negative COVID-19 vaccine side effects.
The group, “COVID19 VACCINE VICTIMS AND FAMILIES,” had over 120,000 followers when it was shut down and had been gaining more than 10,000 followers per week.
Not only is Facebook restricting a wide range of vaccine-related claims but it’s also adding labels to all posts about coronavirus vaccines. These labels state that vaccines are safe and direct users to sources that Facebook has deemed “authoritative” such as the World Health Organization (WHO).
These crackdowns on vaccine skeptic conversations come amid mass pushes from global governments to introduce digital vaccine passports that force people to prove their vaccination or test status to enter business premises.
Published: April 17, 2021 Select LanguageCzechDutchEnglishFrenchGermanGreekHebrewHungarianItalianJapaneseKoreanPolishPortugueseRussianSpanishSwedishTurkishPowered by
The only two exceptions to this rule are extreme lockdowns in China and preemptive lockdowns in support of early border controls, which succeeded primarily on some islands and possibly in Indochina (Vietnam, Thailand, Laos, Cambodia), Norway and Finland. Note that New Zealand and some other islands had already avoided the 1957 and 1968 flu pandemics. Some of the most successful islands never even had a Western-style lockdown (e.g. Taiwan and Japan).
In contrast, lockdowns have caused unprecedented social and economic devastation, destroying hundreds of millions of livelihoods worldwide, according to official estimates. In sub-Saharan Africa, the increase in deaths from malaria and tuberculosis each exceeds the total number of covid deaths. Interestingly, if one takes into account both GDP loss and new public debt, New Zealand is one of the worst affected countries in the world.
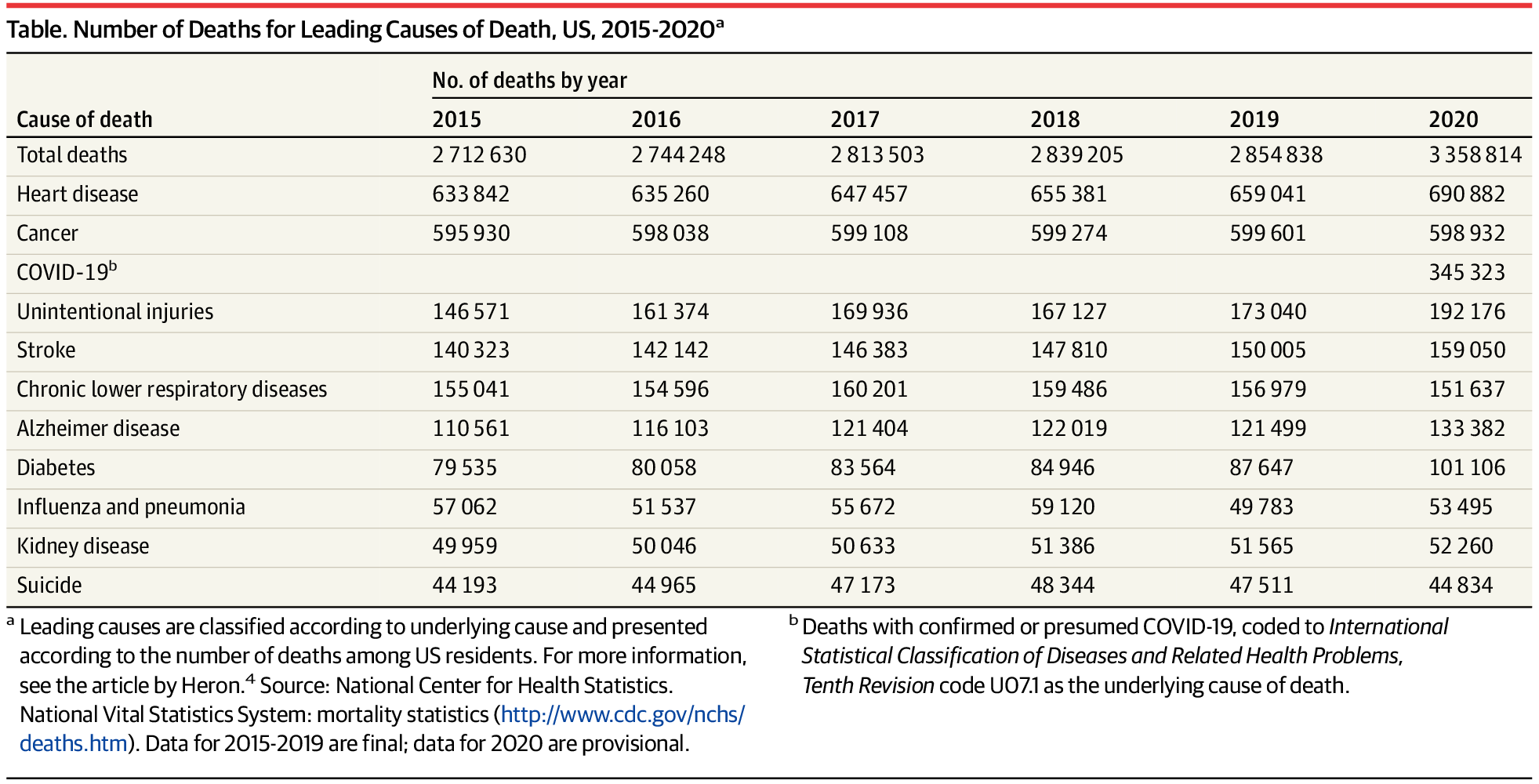
Nevertheless, some proponents of lockdowns argue that lockdowns have at least not led to an increase in suicides. They point to a recent US study, published in JAMA, apparently showing a decrease in US suicides in 2020 by 2,700, from 47,500 to 44,800 (see the table above).
But the reality is far different. First, US CDC data shows that 6,900 cases of “intentional or unintentional injuries”, which include suicides, were classified as “covid deaths” (deaths with covid). But more importantly, suicides in the US cover only a fraction of ‘deaths of despair’: the very same JAMA study shows that “unintentional injuries”, “largely driven by drug overdose deaths”, increased by an unprecedented 19,000 to a sad record of 192,000 (see the table above). And if the economic and labor market situation doesn’t recover quickly, this may have been only the beginning.
Finally, this calculation doesn’t even include the dramatic increases in severe depression and attempted suicides, especially in children and young adults, the groups least affected by covid.
Published: April 2021 (upd.) Share on: Twitter / Facebook Select LanguageCzechDutchEnglishFrenchGermanGreekHebrewHungarianItalianJapaneseKoreanPolishPortugueseRussianSpanishSwedishTurkishPowered by
Did China stage the early videos of people collapsing in Wuhan?
Already in March 2020, SPR argued that the coronavirus situation appeared to show aspects of a possibly serious pandemic, a mass psychosis, and a psychological (i.e. propaganda) operation.
Since the early days of the pandemic, many people have been wondering if the notorious videos of “people collapsing in Wuhan”, which emerged in late January 2020 (see below), had in fact been staged by the Chinese government to frighten the West into lockdowns and self-destruction. After all, it is argued, such events haven’t been seen anywhere else later on during the pandemic.
For instance, on January 31, 2020, British newspaper The Guardian titled: “A man lies dead in the street: the image that captures the Wuhan coronavirus crisis”. A week before, the British Express titled: “Coronavirus horror: Social media footage shows infected Wuhan residents ‘act like zombies’”.
But an analysis of these videos and their context shows the following:
Contrary to claims that there were “dozens” or even “hundreds” of such videos, there were only about ten such videos, which were shown in various places and in various combinations.
Most of these videos really had nothing to do with covid. Rather, these videos showed drunk people, homeless people, road accidents, unspecified medical emergencies, and even training exercises. Some of these videos were quickly debunked by Western “fact checkers”.
Because of the simultaneous virus outbreak, first responders in Wuhan often already wore protective equipment (the white bio-hazard suits). Thus, to bystanders and to people uploading and sharing the videos, it may have looked like actual “sudden coronavirus deaths.”
In many cases, video titles or descriptions suggested or claimed the videos showed “sudden coronavirus deaths”, but in no case was this suggested or claimed by Chinese authorities; instead, it was social media and Western media promoting this frightening narrative.
It looks like most of these videos were shared internationally not by people close to the Chinese regime, but by people and groups opposed to the Chinese regime (e.g. by ‘Voice of Hong Kong’ and ‘Badiucao’), who wanted to show that the Chinese regime had lost control. The video compilation below, for instance, was published by Taiwan-based news platform TomoNews US.
If any of these videos really showed someone collapsing due to the coronavirus, it may have been due to a sudden cardiac arrest caused by viral myocarditis (heart muscle inflammation), or a major heart attack, stroke, or embolism. Such cases have been observed even in the US and in Germany.
Furthermore, it is noteworthy that the first English-language mention of the alleged “Chinese whistleblower doctor” Li Wenliang (who later died or disappeared) came from “China Change”, an “NGO” funded by the US National Endowment for Democracy (NED), a US government controlled entity that sponsors opposition groups in adversarial countries.
This again might indicate that Western state actors either tried to leverage the situation in China, or tried to “frame” China (the real origin of the virus remaining unknown to this day). In contrast, the Chinese government itself primarily tried to downplay the situation, and continues to do so.
While antibody data indicates that by April 2020, coronavirus prevalence outside of Wuhan city and Hubei province was near zero (despite domestic travel in January 2020), China has experienced repeated local outbreaks and continues to impose extreme lockdown and quarantine measures.
In conclusion, there is currently no evidence that the “collapsing people” videos of January 2020 were a “Sun Tzu style” Chinese psyop. Instead, they may have been part of the “mass psychosis” at the time, leveraged by clickbaiters and hoaxers and Western media, or they may have been part of a Western psyop against China, against the Western population, or both.
Postscript
Chinese coronavirus measures, such as disinfection of public places, construction of dedicated field hospitals and quarantine facilities, and early use of ventilators, were based on epidemic response plans developed after the 2003 SARS epidemic and aimed at preventing aerosol transmission. Although extreme and partially ineffective, these measures weren’t part of a deception, either.
It has been argued that Western lockdowns had been promoted by “Chinese Twitter botnets”. However, while it is true that social media botnets were promoting lockdowns, it remains unclear who was operating these botnets. For instance, during the “Russiagate” campaign, US cybersecurity contractors were running “Russian botnets” to influence US state elections.
Video compilation: “Coronavirus has people keeling over in streets” (January 2020)
Former NKVD chief Nikolay Yezhov got removed from a photograph with Stalin, though not for asking questions about vaccine adverse events (Read more; source of meme)
Published: May 6, 2021 Select LanguageCzechDutchEnglishFrenchGermanGreekHebrewHungarianItalianJapaneseKoreanPolishPortugueseRussianSpanishSwedishTurkishPowered by
Online censorship during the pandemic: situation and solutions.
During the coronavirus pandemic, the well-known manipulation and censorship on major US internet platforms Google/YouTube, Facebook, Twitter and Wikipedia has reached unprecedented levels. The platforms generally claim to enforce WHO and local health authority guidelines, not because they are correct – they were mostly wrong – but because they are deemed “authoritative”.
Some notable examples:
In the United States, YouTube deleted a video of the official Senate testimony of US doctors on the importance of evidence-based early treatment, opposed by the US FDA, NIH and CDC.
In Germany, Google and YouTube silently removed ironic anti-lockdown videos by German TV actors from their search results (a classic Google/YouTube manipulation technique). Prior to that, YouTube had already deleted some of the largest independent German media channels.
In Switzerland, in what may have been a world first, Swiss authorities apparently told YouTube to delete five minutes of a live stream – without notifying the streamer – that showed how Swiss police trapped and detained an independent journalist during an anti-repression protest.
Facebook deleted a group with 120,000 members reporting and discussing covid vaccine adverse events and notoriously adds “vaccines are safe” notes to posts of people mourning the post-vaccination death of a family member.
Wikipedia, whose mostly anonymous editors and administrators have repeatedly been exposed as employees or PR agents of pharmaceutical corporations (or British intelligence operatives), has pushed official misinformation and deleted dissent throughout the pandemic.
The solution to this situation is quite simple, however. Advanced internet users should never use Google search, on any device, unless they want to monitor the current extent of censorship; they should never use the internet without an ad and tracking blocker; and they should always try to use alternatives to YouTube, Facebook and Twitter, both as content producers and as consumers.
During the coronavirus pandemic, censorship has affected science itself. For instance, three major journals refused to publish the Danish randomized controlled trial that found no significant effect of face masks against coronavirus infection; another journal refused to publish a meta-analysis on ivermectin-based early treatment that had already been peer-reviewed; and ResearchGate removed a critical review on face masks and deleted the account of its author, a Canadian professor.
The Howard Springs quarantine facility in the Northern Territory of Australia (ABC)
Published: June 9, 2021 (upd.) Share on: Twitter / Facebook Select LanguageCzechDutchEnglishFrenchGermanGreekHebrewHungarianItalianJapaneseKoreanPolishPortugueseRussianSpanishSwedishTurkishPowered by
The high costs of zero covid.
For more than a year already, both Australia and New Zealand have been largely isolated from the rest of the world. Nevertheless, the Australian state of Victoria and its capital city of Melbourne have recently had to impose yet another preemptive lockdown in order to suppress renewed community transmission of the coronavirus.
If they get really unlucky, the citizens of Victoria will have to spend another local winter season in full lockdown. Moreover, many Australians haven’t been allowed to leave the country since early 2020.
Due to repeated failures of the hotel quarantine system for incoming travelers, both New Zealand and Victoria are currently considering, or already planning, a “purpose-built covid quarantine facility” (see example above), already known from places like Vietnam and China.
New Zealand and Australia are also facing a high pressure to quickly vaccinate a very large part of their population, but the vaccines currently in use are already somewhat ‘outdated’ and sub-optimal in terms of their effectiveness against some of the new coronavirus variants, and local reports of blood clots, Guillain-Barré syndrome and other serious vaccine adverse events are mounting.
While it is true that in terms of coronavirus disease, Australia and New Zealand are high-risk populations – due to very high rates of obesity and metabolic disease – the economic and societal costs of lockdowns and isolation have also been substantial. In fact, if one considers both GDP loss and new public debt, New Zealand is one of the worst affected countries in the world. Moreover, in Australia, the number of suicide attempts among children and young adults has doubled.
Meanwhile, China itself is also facing renewed coronavirus outbreaks in several parts of the country, and authorities have again imposed some very strict lockdowns on major cities, despite having already vaccinated hundreds of millions of people – see our updated video gallery (18+) showing recent lockdowns, quarantine facilities and mass vaccinations in Chinese cities.
“Zero covid” essentially means “zero mistakes”, and such a goal was simply unrealistic for most non-island countries in the world (and even for many islands). Furthermore, in early 2020 it was far from certain that an effective vaccine would already become available by the end of the year.
At any rate, the examples of New Zealand and Australia show that “zero covid” is entirely unfeasible without early and strict border controls. Indeed, “zero covid” was unattainable even for most Asian countries, including India, Nepal, Malaysia, the Philippines and Indonesia. For instance, Indonesia had a seroprevalence of about 15% by January 2021, comparable to many Western countries.
There are only a few Asian outlier countries remaining, such as Japan, Korea, Taiwan and the Mekong countries of Thailand, Vietnam, Cambodia and Laos. In these countries, the coronavirus has been circulating at a low level, but there have so far been no major, nation-wide outbreaks.
Omicron neutralization: vaccination vs. vaccination + infection (Sigal)
Published: December 8, 2021 (upd.) Share on: Telegram / Twitter / Facebook Select LanguageCzechDutchEnglishFrenchGermanGreekHebrewHungarianItalianJapaneseKoreanPolishPortugueseRussianSpanishSwedishTurkishPowered by
Important new data on Omicron neutralization in vaccinated vs. recovered people.
Professor Alex Sigal of the African Health Research Institute in Durban, South Africa, has presented the first data on Omicron neutralization in Pfizer vaccine study participants, both with and without previous infection (see preprint study).
As the figure above shows, Omicron neutralization in vaccinated people without prior infection (red) decreased to very low levels (a 41-fold decline compared to the initial Wuhan D614G variant). In contrast, neutralization in previously infected plus vaccinated people (green) remained relatively high and is “likely to confer protection from severe disease”, according to the authors.
Recovered people without vaccination have not been considered in this study, but previous studies found no significant benefit of vaccination in recovered people. Moreover, a recent Dutch study found that “in contrast to vaccine-induced immunity, no increased risk for reinfection with Beta, Gamma or Delta variants relative to Alpha variant was found in individuals with infection-induced immunity.”
Regarding the new Omicron study, three additional aspects are noteworthy:
1) The plasma of vaccinated people was taken on average just 12 days post-vaccination, i.e. at the point of highest antibody levels and neutralization effectiveness (see table below). In people vaccinated months ago, neutralization may no longer be detectable (see updates below).
2) In previously infected people, the plasma was taken a full 417 days post-infection and 27 days post-vaccination, on average (see table below). Despite this, previously infected people still had much higher neutralization levels.
3) In this Pfizer vaccine study, previously infected people had been infected during the first South African wave, which was dominated by the initial Wuhan D614G variant without any antibody escape mutations. However, the second South African wave was dominated by the Beta variant, which features both a class 1 (K417N) and a class 2 (E484K) antibody escape mutation (see table below). Thus, people previously infected with the Beta variant are likely to have even stronger protection against Omicron, which features escape mutations against antibody classes 1, 2, and 3.
This extra-protection may also apply to people in Latin America who were previously infected with the Gamma (Brazilian) variant, but not to people in the US and in Europe who were infected with the Wuhan/D614G (2020), Alpha (spring 2021) or Delta (summer 2021) variant.
In addition, previously infected people may benefit from mucosal and T-cell immunity, which could not be taken into account in the current South African study, either. While it has been reported that PCR-positive hospitalizations in South Africa are currently increasing again, it should be noted that a full 76% of these patients were in fact hospitalized not due to covid.
There have been reports that Omicron might be milder than previous variants. While this would be fantastic news, one should take into account that these reports are based primarily on 1) people in South Africa, most of whom already have natural immunity from previous infection (60% to 80% of the population; only 25% vaccination rate), and 2) non-elderly people (e.g. travelers), in whom covid has always been rather mild anyway (despite relentless propaganda to convince you otherwise).
The question of disease severity can only really be answered once Omicron reaches high-risk groups. In general, the fact that Omicron is able to displace Delta (even in Europe) indicates that Omicron is currently at least as transmissible as Delta, which in turn requires rather high peak viral loads and infectiousness. Unless other mutations reduce host impact, this would not indicate lower virulence. Instead, it is reasonable to assume that virulence may be similar to previous variants.
In conclusion, unless Omicron turns out to be much milder than previous variants, it is evident that current covid vaccines will have to be updated. The fact that current vaccines are no longer effective against Omicron (based on EUA standards) also means that any existing “vaccine passport” schemes and vaccine mandates have become obsolete and have to be suspended immediately.
Ultimately, only widespread natural immunity will be able end the covid pandemic. The fact that millions of “unvaccinated” people are currently being threatened with losing their jobs, regardless of their actual immunity status, can only be described as a crime against humanity. Moreover, the fact that young people have been pressured to take an experimental – and now ineffective – vaccine, against a virus that poses very little risk to them, can only be described as a major medical crime.
Finally, the arrival of immune-escape variants once again highlights the importance of early outpatient treatment of high-risk covid patients, regardless of their vaccination status.
∗∗∗
Update I: A new German analysis confirms 0% neutralization six months after vaccination with Astra-Zeneca, Biontech or Moderna, and only 25% three months after a Biontech booster (vs. 95% against Delta). Furthermore, available monoclonal antibodies show no effectiveness against Omicron.
Update II: A new Swedish Omicron neutralization study in 17 previously-infected hospital workers and 17 recent blood donors in Stockholm found that neutralization was only about 7-fold lower compared to the original Wuhan variant. Given that Stockholm has an infection rate of about 75%, this study again confirms the robust protective effect of naturally-acquired immunity.
Update III: Many news reports argue that the South African, Swedish and German Omicron neutralization studies appear to contradict each other. But as the analysis above shows, this is not the case: rather, the studies differ in terms of previous infections (yes/no) and date of plasma sample (shortly after vaccination vs. six months after vaccination).
Update IV: Independent genetic researchers note that the Omicron variant, with its many spike protein mutations, might in fact have escaped from the Durban lab in South Africa, which has been involved in immune escape and serial passaging cell culture experiments for quite some time.
Update V: A 40-fold reduction in neutralization is not equivalent to a 40-fold reduction in vaccine effectiveness. However, previous studies have shown that “neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection”. Based on the available data, one can estimate that the current Pfizer vaccine will achieve an effectiveness against symptomatic infection of at most 30%. Effectiveness against severe disease may or may not be higher. In the worst case, non-neutralizing antibodies might even enhance infection (ADE).
Figures
A) South African study – participant data
Participant data of the South African Omicron study (Sigal)
B) SARS-CoV-2 Antibody Escape Mutations
Coronavirus variants: Escape from antibody classes 1 to 3 (SPR, based on Greaney et al.) Example: K417N describes an amino acid change at codon position 417 from lysine (K) to asparagine (N).
C) Calculated antibody binding to coronavirus variants
Calculated antibody binding to coronavirus variants (Bloom lab)
D) Neutralization vs. vaccine effectiveness
Neutralization vs. protection against Delta and non-Delta (Gardner et al)
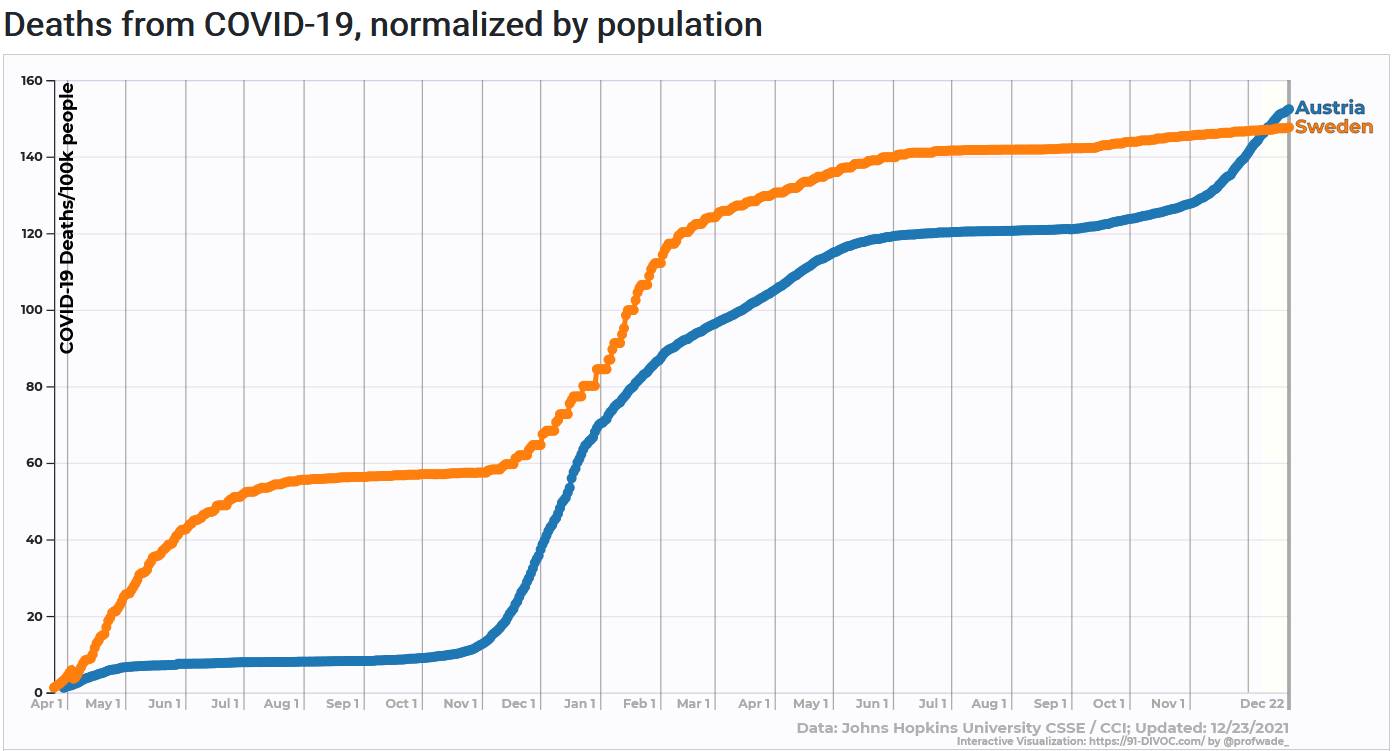
Total covid mortality: Sweden vs. Austria (JHU/CSSE)
Updated: January 3, 2022 Published: December 23, 2021 Share on: Twitter / Facebook / Telegram Select LanguageCzechDutchEnglishFrenchGermanGreekHebrewHungarianItalianJapaneseKoreanPolishPortugueseRussianSpanishSwedishTurkishPowered by
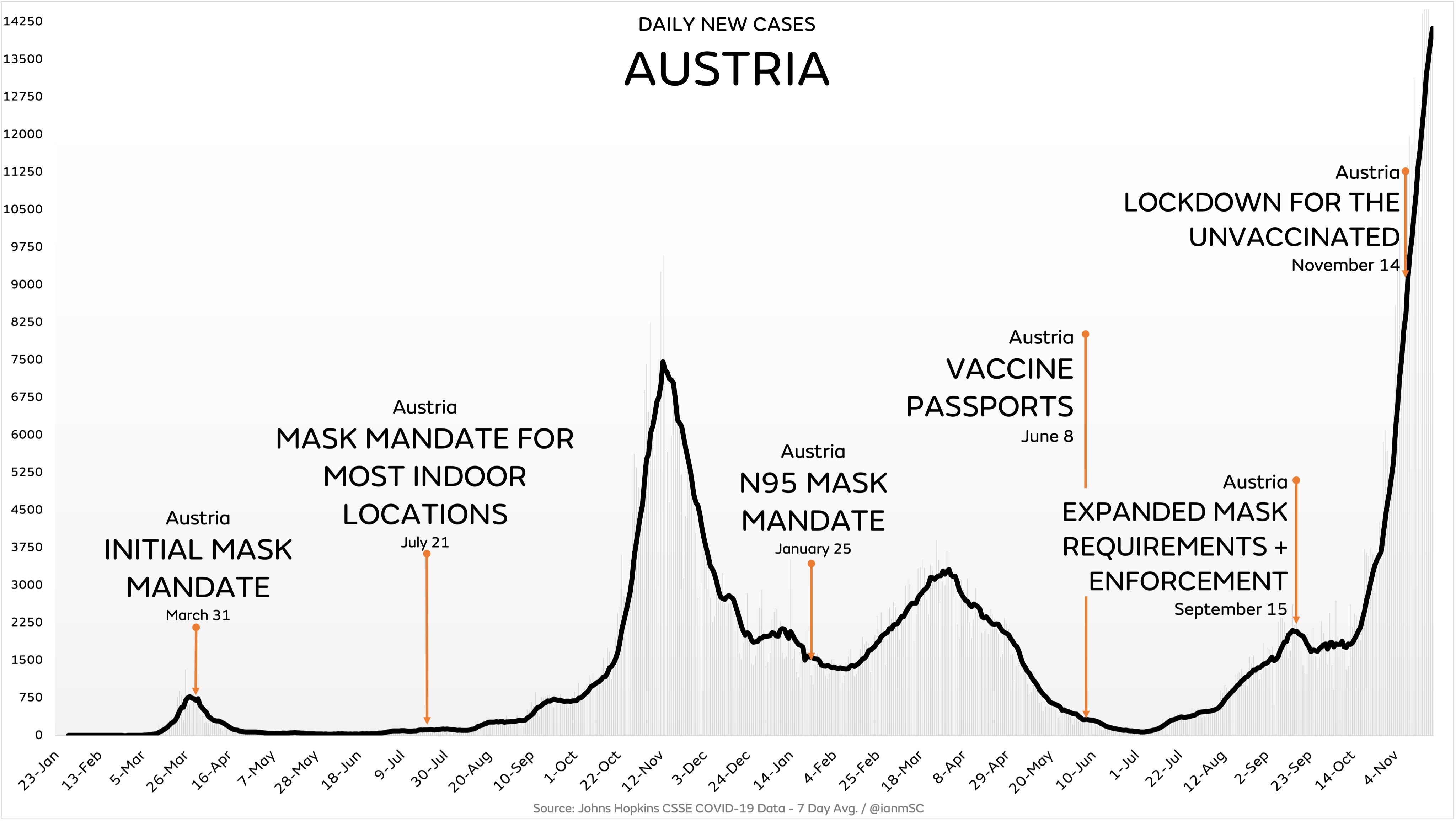
Austria, one of the most repressive European countries during the coronavirus pandemic, has recently overtaken Sweden in terms of total covid mortality, showing that almost all government interventions have been ineffective and unjustified.
Throughout the coronavirus pandemic, Austria has been one of the most repressive European countries, implementing several lockdowns, school closures, far-reaching mask mandates and even an N95/FFP2 mask mandate, record-setting mass PCR testing and contact tracing, as well as early “vaccine passports”. Austria was also the first Western country to impose a “lockdown for the unvaccinated” and the first Western country to announce a general “vaccine mandate”.
In contrast, Sweden has widely been regarded, or indeed criticized, as the least repressive Western country during the coronavirus pandemic, having imposed no lockdowns, no elementary school closures, no mask mandates, no “vaccine passport” (until December), and very limited testing and contact tracing compared to Austria and many other Western countries.
And yet, in December 2021, Austria overtook Sweden in terms of total covid mortality (see chart above). This comes after Austria had reached, in late November, the highest seven-day covid infection rate in the world. The European average covid mortality had already overtaken Swedish covid mortality back in March 2021.
But can Nordic Sweden and Alpine Austria really be compared in a legitimate way? Indeed, they can. To begin with, their population size is quite similar (10.4 million in Sweden vs. 9.0 million in Austria). While the median age in Sweden is slightly lower than in Austria (41.1 vs. 44.4 years; perhaps due to more immigration), the Swedish life expectancy is actually somewhat higher than in Austria (82.4 vs. 81.6 years). Vaccination rates are very similar in Sweden and in Austria (72% vs. 70%).
Interestingly, the population weighted density, which takes urbanization into account, is somewhat higher in Sweden than in Austria (2724 vs. 2191, see map below). The share of single households is also somewhat higher in Sweden than in Austria (40% vs. 36%, both very high figures). Obesity rates are very similar in Sweden and in Austria (20.6% vs. 20.1%). ICU capacity is significantly higher in Austria than in Sweden (5.3 vs. 1.9 beds per 1000 people).
In fact, total covid mortality in Austria and in Sweden may have reached the same level precisely because the two countries are so similar in terms of demographic and health factors. In both countries, the covid population fatality rate (PFR) has reached about 0.15% and is limited primarily to people over 70 years of age (the median age of covid deaths is about 83 years in both countries).
But is it fair to call December 2021 the “judgment day”? Indeed it is, because Sweden has already crossed the “pandemic finish line” and was the first Western country to see the return of influenza, which had been displaced by the coronavirus since March of 2020. Of course, the novel coronavirus will not disappear from Sweden or from anywhere else, and Sweden will certainly see future coronavirus waves, but Sweden has achieved a high population infection rate (about 60% to 75%) and has entered the endemic phase.
Thus, the fact that Austria has now overtaken Sweden in terms of total covid mortality really means that almost every single government intervention in Austria – and almost everywhere else – has been entirely ineffective from an epidemiological and medical perspective, while having caused almost unprecedented social and economic harm.
In particular, it means that lockdowns, school closures, mask mandates, N95/FFP2 mask mandates, mass PCR testing and “contact tracing”, as well as “vaccine passports”, have been entirely ineffective and unjustified as interventions to “combat the pandemic”.
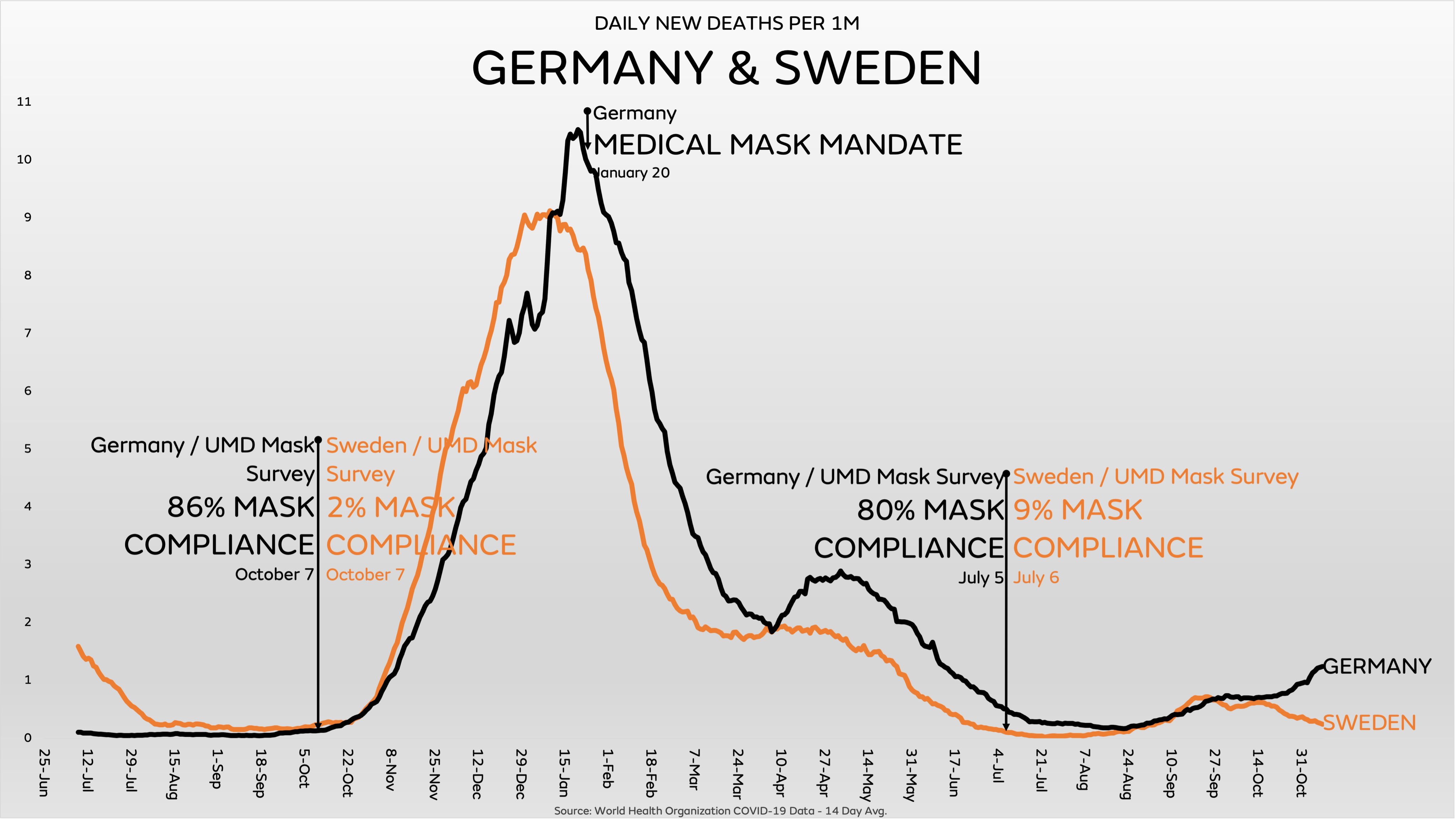
Of note, this is not just “post-hoc knowledge”: with the exception of school closures (which are effective against influenza), it had long been known that all of these “interventions”, including masks and contact tracing, are ineffective against respiratory virus epidemics. Concerning face masks and N95/FFP2 masks, the question is not if they are effective in theory or in some lab experiment, but if they make any difference in the real world – and the answer is no.
In fact, in terms of all-cause excess mortality, Austria had surpassed Sweden already several months ago: total pandemic excess mortality currently is 17% in Austria vs. 11% in Sweden. This is primarily because many Swedish deaths happened earlier in the pandemic (in the spring of 2020) and most covid victims were very old (median age of 83); thus, by September 2020, Sweden recorded its lowest mortality in history. (Nevertheless, claims that Sweden has had no or almost no excess mortality are based on an incorrect calculation method; there is no “Swedish mortality miracle”).
The same result has been observed in many other regions throughout the world: In Eastern Europe, Belarus has recorded an average regional excess mortality despite almost no interventions at all; in Latin America, excess mortality in Brazil has been higher than in Chile and Argentina, but lower than in Peru, Bolivia, Ecuador, Mexico, Colombia and Paraguay; in Asia, lockdowns in India, Indonesia or the Philippines were horrific failures threatening the livelihood of millions of families.
There was only one situation in which lockdowns were a rational intervention: as a preemptive measure in support of early border controls. This situation applied primarily to some islands, such as Australia, New Zealand and Iceland, and possibly to Norway, Finland, Denmark and parts of China (more on these countries below).
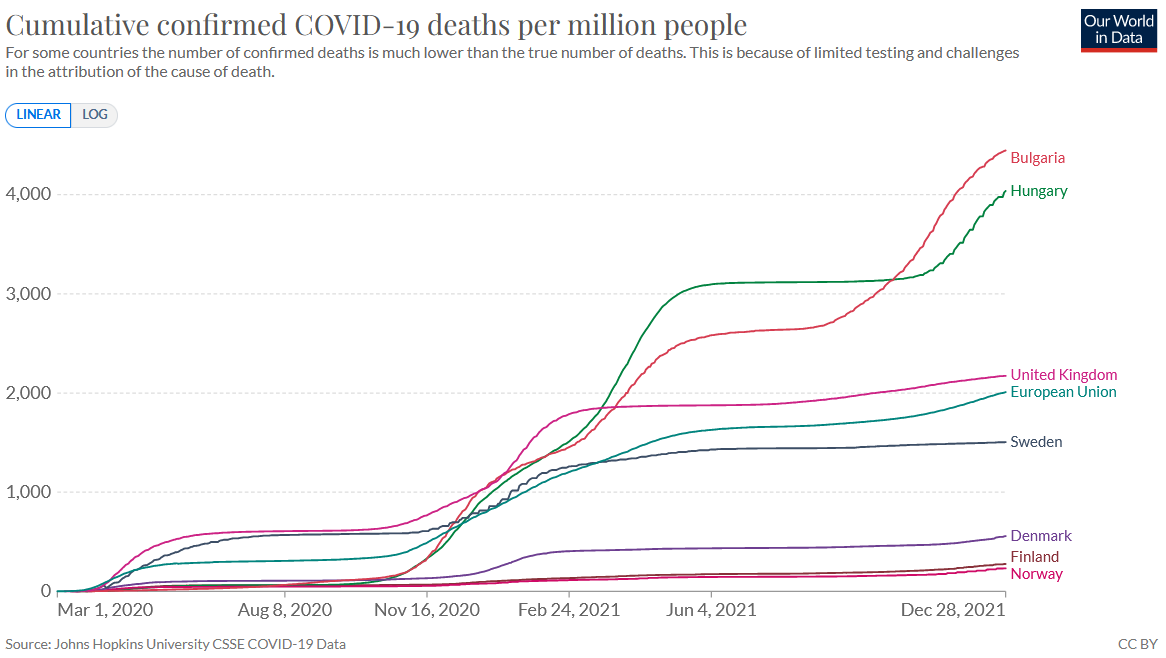
Critics of the Swedish approach have often argued that Sweden should only be compared to “its neighbors”. If one compares Sweden to all of its neighbors in the region – Norway, Finland, Denmark, but also Poland and the Baltic states – Sweden again shows an average covid mortality: Poland, Latvia and Lithuania are much higher, Estonia is similar, while Denmark, Finland and Norway are much lower.
But some critics of Sweden insist on comparing Sweden only to Denmark, Finland and Norway. These critics would like to imply that Sweden is a high-mortality outlier, when in reality, it is Denmark, Finland and Norway which are the true outliers, having by far the lowest covid mortality rates among Western countries. But why is this?
It is not, as critics of Sweden would like to imply, because these countries had particularly strict measures. In fact, for the most part, their “stringency index” was even lower than in Sweden, and of course also lower than in repressive countries like Austria.
Instead, three explanations seem plausible.
First, Denmark, Finland and Norway imposed early border controls and could avoid a major unexpected wave in the spring of 2020. “Early” here is a relative term and always depends on when the coronavirus reaches a certain country. Due to the timing of its winter holidays, the Stockholm area unknowingly imported the coronavirus directly from early covid hotspots in Alpine skiing resorts near Italy, which was not the case in other Nordic countries or even in other regions of Sweden. (In the famous case of Uruguay in South America, the first covid wave hit not until November 2020).
Second, and in the same context, other Nordic countries imposed preemptive lockdowns in support of early border controls that really may have helped disrupt early infections. But a lockdown is ‘preemptive’ only if there have been either no confirmed infections at all or only a very small number of infections that can still be contained before the virus gets aerosolized.
Third, and most fundamentally, Norway and Finland have by far the lowest population weighted densityin Europe (910 in Norway and 986 in Finland, vs. 2724 in Sweden and 6785 in Britain; see the map below), which may have helped slow the spread of coronavirus infections. In this regard, Sweden is indeed closer to countries like Austria (2191) and the Netherlands (2426) than to its direct geographic neighbors Finland and Norway.
In fact, in Western Europe, there is a striking correlation between population weighted density – which may influence both the speed of virus transmission and the amplitude of infection waves – and covid mortality per country (see map below). This correlation does not apply, however, to Denmark, which has a low covid mortality but an average population weighted density (3434).
At the global level, high population weighted density (PWD) might help explain strong covid waves in Britain, Spain and Italy, Turkey, South America (including Mexico) and South Africa, but not (so far) in Japan, Canada, Australia and New Zealand. Low PWD could help explain the slow spread of the coronavirus in Norway, Finland, Indochina, and parts of Black Africa (see map below).
In addition, Scandinavian countries have the highest percentage of single households in the world, which might be seen as a kind of “natural quarantine” that helps protect family members: 45% in Denmark, 41% in Finland, 40% in Sweden, and 39% in Norway. In Austria, it is 36%, in Japan 34%, in Italy 31%, in the US 28%, in Spain and in Portugal 19%, and in Brazil 12%.
Coming back to the comparison of Sweden and Austria, one factor that worked against Austria was the failure of covid vaccines: if covid vaccines had provided strong long-term protection, Austria could have avoided the high covid mortality in the winter of 2021/22. On the other hand, in the spring of 2020, even optimists hadn’t expected covid vaccines becoming available before autumn 2021.
The failure of covid vaccines is also a major problem for low-covid countries like Norway, Finland, Denmark, Australia, New Zealand and China, which now are in a rather uncertain position.
While all of the interventions imposed by Austria and other repressive countries failed, are there any potentially effective interventions that have not been adopted?
A few options may be mentioned.
First, research and use of repurposed early treatment drugs should have been a major priority to reduce hospitalizations (especially given the uncertainties regarding vaccine protection).
Second, dedicated covid hospital facilities should have been created to avoid widespread in-hospital transmission (in some countries, including Sweden, the UK and the US, such facilities were indeed created, but they remained largely unused).
Third, given their low covid risk, offering voluntary, medically supervised live virus infection to children and young healthy adults may have made sense to rapidly build up a natural immunity shield, protect high-risk groups (including parents), and ensure smooth education.
Fourth, while masks have been a complete failure (as was already known before the pandemic), indoor ventilation to prevent aerosol transmission might have been one of the most effective interventions (with >99% of all transmission occurring indoors). Then again, living rooms and class rooms cannot be turned into airplane cabins.
Fifth, the media should have supported the calm management of the pandemic, fostering social cohesion and mindfulness, instead of inciting panic and hysteria, which caused large parts of the public to overestimate covid mortality by a factor of one hundred. The many “dashboards” and “live tickers” may well have been counterproductive, too.
Sixth, we may have to recognize that societies with a life expectancy of over 80 years and obesity rates of over 20% are inherently susceptible to events like the coronavirus pandemic. Care home residents, who accounted for about 50% of Western covid deaths, should have deserved a more humane treatment during their last remaining months on earth.
Needless to say, most Western health authorities have not yet acknowledged that their entire approach to the pandemic has been a complete failure. As a case in point, the Austrian health minister in early December claimed that the most recent Austrian lockdown had been effective in breaking the winter wave, but independent analysts quickly pointed out that infections had decreased simultaneously in neighboring countries without a lockdown.
In conclusion, the comparison of Austria and Sweden conclusively shows that a calm, low-intervention and patient-focused approach to the pandemic has been best. In contrast, epidemiologically irrational strategies, such as “zero covid” and “no covid”, have caused unprecedented social, political and economic damage at an almost civilizational scale.
You have been reading: Judgment day: Sweden vindicated. An analysis by Swiss Policy Research.
Postscript
In the United States, California – one of the most restrictive states – has recently overtaken Florida – one of the least restrictive states – in terms of age-adjusted all-cause excess mortality:
California vs. Florida: age-adjusted excess mortality (US Mortality)
Figures
A) Population weighted density in Western Europe (2015)
The analysis above quotes 2020 figures, while the following map shows 2015 figures.
Population weighted density in Western Europe (2015) (WorldPop)
B) Global population weighted density (2020)
Global population weighted density (2020) (WorldPop)
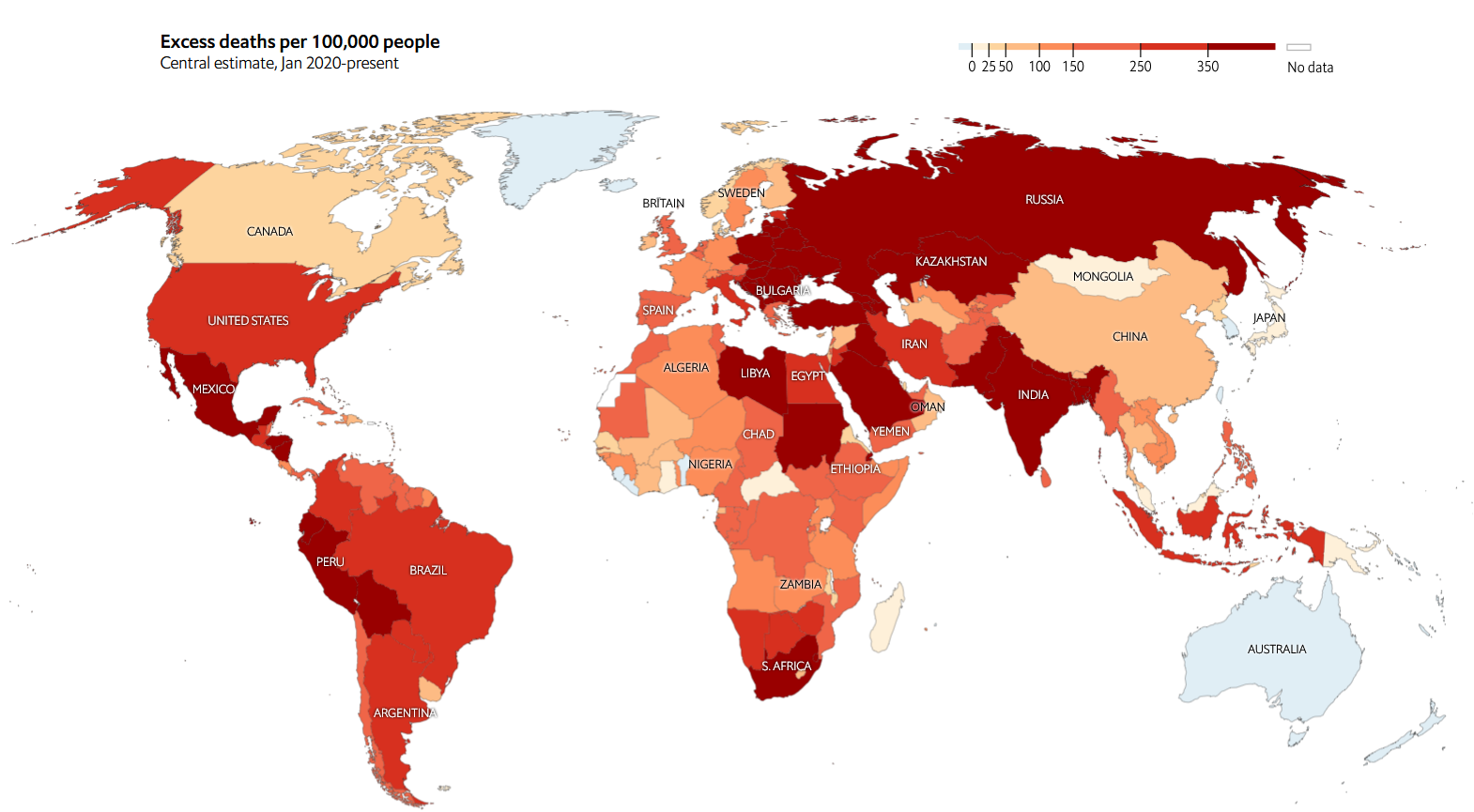
C) Excess mortality per country (January 2020 to December 2021)
Excess mortality per country (January 2020 to December 2021) (Economist)
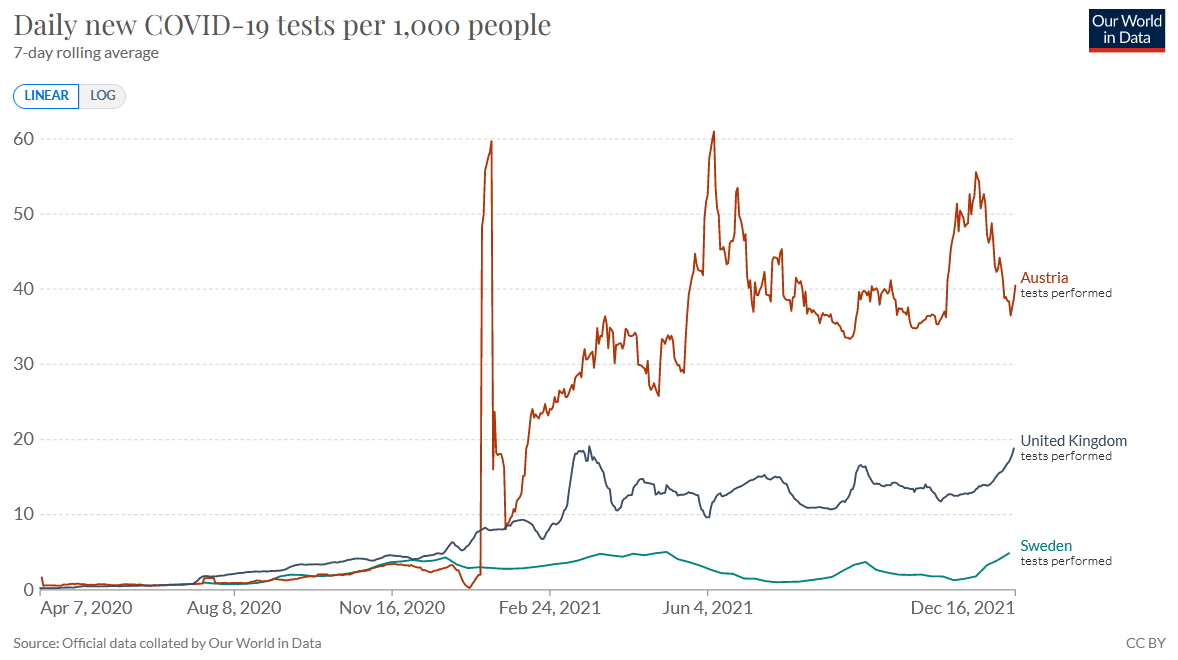
D) Daily covid tests per 1000 people
Daily covid tests per 1000 people in Austria, Sweden and Britain.